
If you wanted to produce a movie about a controversy in audiology, then binaural amplification might be the subject with the most plot twists and turns. Essentially, it has all (okay, maybe just some!) of the key movie elements found in a science thriller: legendary hearing researchers indicating binaural aids weren’t particularly beneficial; leading hearing aid specialists saying they were; more legendary researchers and clinicians re-assessing the question and coming to new conclusions—all against a backdrop of finger-pointing and accusations about self-interests and profits, as well as a pivotal ruling by the Supreme Court. Lights, Camera, Action!
Act 1: Challenges and Questions about Binaural Benefit
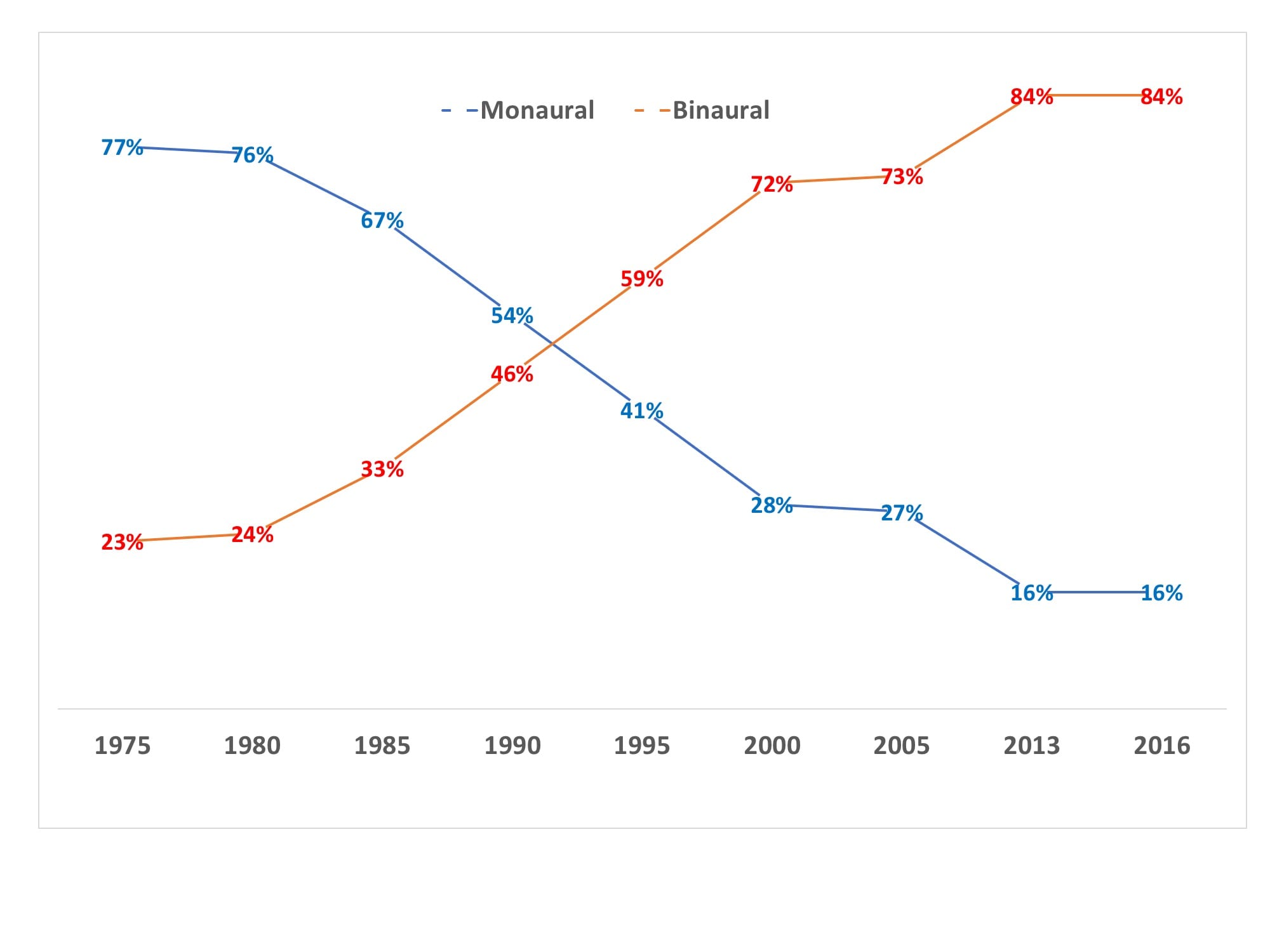
Binaural hearing aid fittings have completely changed the hearing healthcare landscape for the better. However, the road to this particular “best practice”—with probably around 85% of all of today’s fittings involving two hearing aids—was not a smooth one in the United States. Figure 1 shows that fewer than one-quarter of all US hearing aids fit prior to 1980 were binaural, and controversies swirled around the benefit of binaural fittings well into the late-70s. It should be acknowledged that monaural eyeglass aids were a very popular style in the 1960s, and may have complicated the debate. Additionally, prior to 1978, the role of the audiologist was to test and recommend hearing aids, but not dispense the devices. This probably added to some “disconnect” between clinical audiology and practical dispensing.
There were some who believed binaural fittings were downright unethical and motivated by profit. Indeed, when looking back, they had some reason for concern. Several studies using test methods of that time did not support binaural hearing. In particular, a 1961 study by three bona-fide legends in audiology research—Raymond Carhart, James Jerger, and Donald Dirks—published in two papers described their findings as “remarkably unsuccessful in demonstrating objectively that the hearing impaired derive any significant gain in speech intelligibility from binaural as opposed to monaural hearing aids.”1,2 However, as Mark Ross later pointed out, the word score tests in this early study were performed in monaural direct orientation, a condition we would now expect to differ least from the binaural scores.3
Yet, even 15 years later, the final 1977 report to the US Federal Trade Commission (FTC) by the Bureau of Consumer Protection was rather equivocal, at best:
“Binaural amplification is generally considered appropriate only for people with a relatively symmetrical hearing loss, although some industry representatives dispute the point. Manufacturers and dispensers are understandingly enthusiastic supporters of binaural amplification, since it means the sale of two hearing aids rather than one. Audiologists are less enthusiastic, principally, because of the dearth of clinical evidence of binaural superiority. The advantages cited for binaural amplification include improved localization ability, better speech discrimination ability, greater ease of listening and better sound quality. These advantages are essentially subjective and therefore cannot be demonstrated with existing clinical techniques.”4
Act 2: Evidence Mounts for Binaural Fittings
Advances in clinical testing and emerging evidence for the binaural advantage continued throughout the 1970s-80s. For example, two alumni from Brooklyn College, audiologists Earnest Zelnick and John Duffy, published papers5,6 on the benefits of binaural amplification in children. Other researchers in the mid-70s like Nabelek and Pickett7 and Dermody and Burne8 pointed out the advantages of hearing in noise with binaural aids, setting the stage for later research on the binaural advantage with directional microphones (eg, Hawkins and Yucullo in 1984).9
Related Article: The Search for the Binaural Advantage…Revisited, by Cy Libby (Nov 2007 HR)
In 1980, E. Robert “Cy” Libby published an extremely influential monograph, Binaural Hearing and Amplification,10 featuring some of the most prominent researchers of the day. In short, the evidence for binaural amplification had become overwhelmingly persuasive. However, as Libby pointed out in his November 2007 Hearing Review retrospective,5 nothing less than the US Supreme Court came to the rescue in finally settling the monaural-binaural debate: in 1978, the Court ruled on a case that indirectly forced the American Speech-Language-Hearing Association (ASHA) to lift its ban on hearing aid dispensing for audiologists. Following this decision, many members of ASHA who had previously been critical of binaural amplification became dispensing audiologists and discovered the binaural advantage on their own.
The transformation was so complete that, by the late-1980s, papers were being published in the ASHA journal about why not recommending binaural amplification for applicable patients might constitute malpractice.11 Additionally, by the early-1990s, researchers like Moore and Silman et al were addressing the potential negative effects of auditory deprivation in monaural fittings.12,13
Act 3: Cataloguing and Explaining the Binaural Advantage
When a patient asks an HCP, “Do I really need two hearing aids?”, the typical response is something like “Yes, because you have two ears.” The real answer, of course, is much more complicated. Stender14 listed four key reasons why a binaural fitting is superior:
- Better localization abilities, or the ability to decipher the location of sound sources;
- Improved speech intelligibility in noise, in part due to better spatial release from masking;
- Prevention of auditory deprivation of the unaided ear, when that ear also has aidable hearing loss, which may result in decreased speech recognition for the unaided ear; and
- Possible relief from tinnitus.
Similarly, Kochkin and Kuk15 provided a 15-point list of possible binaural hearing aid benefits:
- Better understanding of speech;
- Better understanding in group and noisy situations;
- Better ability to tell the direction of sound;
- Better sound quality;
- Smoother tone quality;
- Wider hearing range;
- Better sound identification;
- Keeps both ears active resulting in less hearing loss deterioration;
- Hearing is less tiring and listening is more pleasant;
- Feeling of balanced hearing;
- Greater comfort when loud noises occur;
- Reduced feedback and whistling;
- Tinnitus masking;
- Consumer preference, and
- Customer satisfaction.
Act 4: Towards More Patient-centric Hearing Aid Selection Protocols
Even given all of these recognized binaural benefits, there remain patients who not only prefer but also benefit most from a monaural fitting, possibly due to deficits in central auditory processing.16 For example, Mussoi and Bentler17 showed that about 1 in 6 people (16.7% of all listeners, and higher for older adults) present with binaural interference—the condition of poorer speech recognition when listening with two ears versus one ear. Although this should not dissuade HCPs from recommending binaural hearing aid fittings, it does call attention to the need for being mindful that some people have a real and logical preference for using only one hearing aid. The researchers recommended bilateral speech-in-noise testing with adaptive levels of background noise (eg, HINT) to assess the viability of monaural hearing aid use.
Related article: Symposium Reviews 25 Years of Binaural Hearing Research (February 2006 HR online)
Beyond central processing or binaural interference, the other most obvious negative aspect to a binaural fitting is cost. Two hearing aids are more expensive than one, and affordability is a key component in acceptance of a recommendation for a hearing solution. Having a range of economical amplification options and flexible financing—like the program offered by Ally Lending—can help more patients accept recommendations for binaural fittings.
Seventy years ago, Licklider wrote “We must take into account that man’s auditory system has two input channels.”18 We have two ears for a reason. The second ear isn’t simply for back-up or a system redundancy, any more than your right eye exists because you might poke out your left. This fact certainly hasn’t been lost on today’s researchers and developers of hearing aids. The binaural revolution has been a boon for HCPs, the hearing industry, and most importantly, consumers who have benefitted enormously from the binaural advantage. With ever-improving directional technology, wireless streaming, innovative speech-in-noise algorithms, and new auditory science, we can end this monaural-binaural historical drama on a high note: the best is yet to come.
References
- Jerger J, Carhart R, Dirks D. Binaural hearing aids and speech intelligibility. J Speech Hear Res. 1961;4:137-148.
- Jerger J, Dirks D. Binaural hearing aids, an enigma. J Acoust Soc Am. 1961;33(4):71-74.
- Ross M. Binaural versus monaural hearing aid amplification for hearing impaired individuals. In: Bess F, ed. Childhood Deafness: Causation, Assessment & Management. New York: Grune and Stratton; 1977.
- Hearing Aid Industry Staff Report. Final Report to the FTC and Proposed Trade Regulation Rule (16 CFR Part 440). Washington, DC: Bureau of Consumer Protection; September 1978.
- Zelnick E. Comparison of speech perception utilizing monotic and dichotic modes of listening. J Auditory Res. 1970;10:87-97.
- Duffy JK. Binaural hearing aids for children. In: Libby ER, ed. Binaural Hearing and Amplification: Volume II. Chicago: Zenetron Inc; 1980:217-228.
- Nabelec AK, Pickett JM. Monaural and binaural speech perception through hearing aids under noise and reverberation with normal and hearing-impaired listeners. J Speech Hear Res. 1974[Dec];17(4):724-739.
- Dermody P, Byrne D. Auditory localization by hearing impaired persons using binaural in-the-ear hearing aids. Brit J Audiol. 1975;9:93-101.
- Hawkins D, Yacullo W. Signal-to-noise advantage of binaural hearing aids and directional microphones under different levels of reverberation. J Speech Hear Disord. 1984;49:279-286.
- Libby ER. Binaural Hearing and Amplification: Vol 1 & 2. Chicago: Zenetron, Inc;1980.
- Lowe G. Are audiologists guilty of malpractice if they do not recommend binaural amplification? ASHA. 1988;30(11):39-40.
- Moore DR. Plasticity of binaural hearing and some possible mechanisms following late-onset deprivation. J Am Acad Audiol. 1993;4:277-83.
- Silman S, Silverman CA, Emmer MB, Gelfand SA. Adult-onset auditory deprivation. J Am Acad Audiol. 1992;390-396.
- Stender T. On the benefits of binaural. Hearing Review. 2014;21(7):28-31.
- Kochkin S, Kuk F. Binaural hearing aids: The fitting of choice for bilateral loss subjects. Available at: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.482.7726&rep=rep1&type=pdf
- Arlinger S, Gatehouse S, Kiessling J, Naylor G, Verschuure H, Wouters J. The design of a project to assess bilateral versus unilateral hearing aid fitting. Trends Amplif. 2008 [Spring]; 12(2):137–144.
- Mussoi BSS, Bentler RA. Binaural interference and the effects of age and hearing loss. J Am Acad Audiol. 2017 Jan;28(1):5-13. doi: 10.3766/jaaa.15011.
- Licklider JCR. Basic correlates of the auditory stimulus. In: Stevens SS, ed. Handbook of Experimental Psychology. Wiley Publishing;1951:985-1039.
About the author: Karl Strom is editor-in-chief of The Hearing Review and has been reporting on hearing-related issues for over 25 years. He wrote this article for the sponsored Ally Lending enewsletter.

Loved it with being identified in 3rd grade in the ‘60’s with it being unethical to fit two HAs. Then being fit with two in Grad School at University of Iowa., and continuing to pioneer and advocate through the years for better hearing and services for hearing … long recognizing the benefits.