Tech Topic | January 2019 Hearing Review
This study supports the idea that modern hearing aid technology improves patients’ quality of life to a greater extent than shown in previous studies. While it is not possible to determine the degree of the direct relationship, it appears that own voice processing leads to talking more in important communication situations, and, in turn, helps lead to this improvement.
It was back in the early 1990s when the FDA took a hard look at hearing aid advertising in the United States. At the time, there were newspaper and television ads that included speech-understanding-in-noise claims that certainly were not data based, and, in some cases, simply untrue. In April of 1993, letters were sent out from the FDA to many major manufacturers, pointing out misleading promotional material(s) used by that company.
One such letter went to Siemens Hearing Instruments. Siemens did not have misleading speech understanding claims, but, rather, the FDA questioned a consumer brochure that they had produced titled “Better Hearing is Better Living.” Now, to most of us, this statement is rather innocuous and more or less common sense. After all, why wouldn’t better hearing be better living? The unfortunate fact was that, in 1994, there were little data to support this statement.
Since the FDA concerns of the early 1990s, there has been an increase in research on this topic, with two systematic reviews of the literature supporting the quality-of-life (QoL) benefits that hearing aid use provides.1,2 Similarly, one large study on this topic was conducted by the National Council on Aging (NCOA) in the late 1990s.3,4 The assessment of quality of life has also been included in recent large-scale surveys of hearing aid users. For example, Hougaard et al5compare the worldwide findings of the EuroTrak 2015 (ET 2015) and MarkeTrak 9 (MT9)6about hearing loss and hearing aids which examined the non-auditory benefits of amplification. They point out that, among other things, a significant percentage of users report that hearing aids improve their relationships at home. Additional positive findings regarding quality of life have been revealed in the EuroTrak 2018 surveys. But there still remains a need for additional real-world evidence showing that, indeed, hearing aid use improves quality of life.
Documenting Hearing Aid Benefit
As early as the first hearing aid directional microphone research by Maico in 1972,7 it has been common for hearing aid manufacturers to support new technology and algorithms by conducting laboratory measures isolating the feature of interest. Most often this involves some type of speech-recognition measure, judgements of speech quality, or, in recent years, measures of listening effort as a function of the feature activation. This approach is reasonable, as it determines the efficacy of the feature under controlled, near-ideal conditions. But, it’s well recognized that these laboratory measures do not always predict real-world effectiveness.
There are many self-assessment scales that can be used to determine benefit and/or satisfaction with hearing aids in the users’ everyday life. This is a step beyond the controlled laboratory testing and these outcome measures add face validity to the overall evaluation of hearing aids. There is generally agreement between laboratory measures and the real-world assessment by the patient, although this usually only will occur if the assessment scale focuses on the specific feature(s) of the hearing aid under study, and if the benefit observed in the laboratory is large enough to make a real-world difference. For example, very effective bilateral beamforming might show a 5-6 dB SNR advantage in laboratory testing, but this advantage might not be noticeable in the real world if the patient’s lifestyle only involves either very quiet or unusually noisy situations. Additionally, a patient with high expectations may show a large laboratory advantage for a given feature, but still not report adequate satisfaction for real-world listening. It’s clear that we need to evaluate more than just the features themselves.
This takes us back to assessing the impact the use of hearing aids has on the patient’s quality of life. More self-confidence? Better relations around the house? More sociable? A better life overall? As part of a larger study on communication activity following the fitting of hearing aids,8 we examined to what extent a QoL improvement would be noted for new hearing aid users, following 6 weeks of hearing aid use.
Clinical Study
The research was conducted at the Department of Audiology and Speech Pathology, University of Arkansas at Little Rock/University of Arkansas for Medical Sciences. All participants had mild-to-moderate bilateral sensorineural hearing loss, and they were all new hearing aid users. A total of 40 individuals were initially recruited for the larger study.8 The present analysis required that the participant’s significant other also complete the outcome measure, which reduced the sample size to 28 (26 of the 28 significant others were a spouse). The participants in the sub-sample ranged in age from 26 to 94 years (mean age 59.3); there were 14 males and 14 females.
All subjects were fitted bilaterally with the Pure 7Nx RIC hearing aids, with the Nx-fit prescriptive algorithm. Fitting domes/tips were selected to be appropriate for the participants’ hearing loss. All standard special features were activated, including the new Signia Own Voice Processing (OVP) algorithm. Clinical research has shown that OVP improves the naturalness of the user’s own voice when talking, and will increase patient satisfactioin.9-11
At the time of the fitting, each participant filled-out a modified COSI form (Client Oriented Scale of Improvement).12 They were asked to nominate at least three different communication settings that were important to them, where they believed that they could participate more in the conversation. After hearing aid use, they then rated their degree of conversation participation as: Less, Same, Slightly More, More, or Much More. The participants used the hearing aids in the home trial for a total of 6 weeks.
At the end of the 6-week period, the participants also completed a form related to any changes in quality of life that might have occurred since they started using the hearing aids. Categories were selected based on those used in previous research by the National Council on Aging (NCOA), a survey of 2,069 hearing-impaired individuals (1,037 hearing aid users) and 1,710 of their family members, and reported by Kochkin and Rogin.3 Items included in the present study were self-confidence, feelings about myself, relations at home, participation in group activities, social life, and overall quality of life. Each item was rated on a 5-point scale: Worse, Same, Some Improvement, Improvement, Much Improved. This QoL scale was also independently completed by the significant other of the participant, based on their observations of the hearing aid users since they had been using hearing aids.
Available for data analysis, therefore, was the QoL ratings of the participants, a comparison of these ratings to previous studies (eg, the NCOA report), a comparison to the ratings of the significant other, and determination of the relationship between quality of life and the COSI ratings from the larger study.8
Results
The ratings for the 28 participants were initially analyzed based on whether an improvement for any of the situations occurred—that is, a rating of Some Improvement, Improvement, or Much Improved. The percent of these ratings for each item were calculated, and are displayed in Figure 1. Observe that for all items at least 50% of the respondents noted an improvement after using hearing aids for only 6 weeks. The highest rating was for “life overall,” where 19 of the 28 participants (68%) noted at least some improvement. The item that garnered the most “Much Improvement” ratings was Self-Confidence (18% of the participants).
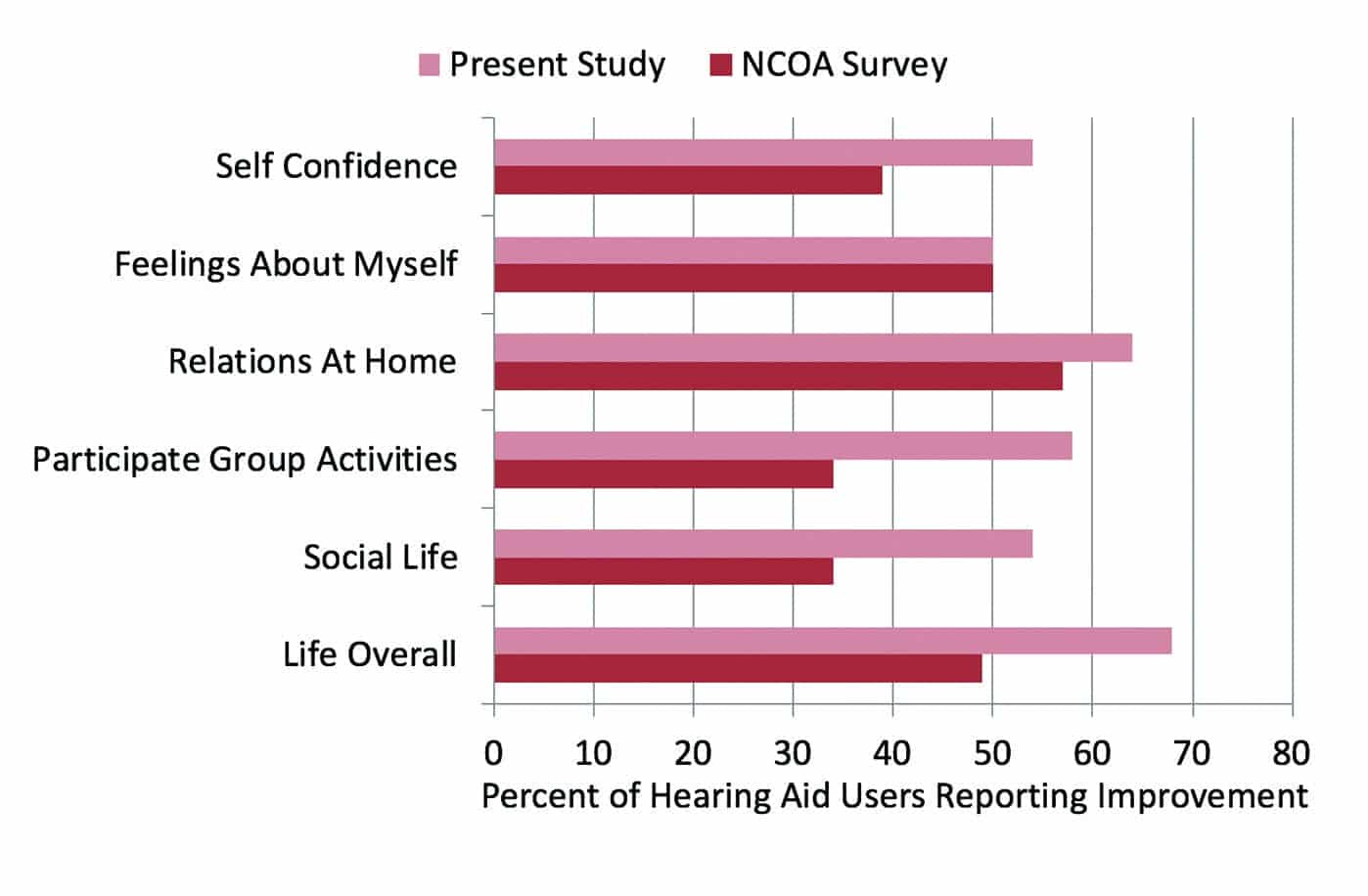
Figure 1. Shown are the percentage of participants who reported at least “Some Improvement” for the different quality-of-life items. Shown for comparison are the findings from the National Council on Aging (NCOA) for the same items.2,3
We are accustomed to seeing outcome measures that are geared toward “hearing,” where it is common that 80-90% of the respondents report an improvement. We must remember, however, that what we are measuring here are quality-of-life issues, where, for many, hearing is a small part of the equation—especially if other, more critical health issues exist. To put the data from this study in perspective, we have included the data from hearing aid users (those with mild-to-moderate hearing loss) reported in the previously mentioned NCOA survey3,4 (see Figure 1). Note that for most dimensions, the percentage of individuals reporting improvement in the present study is substantially higher than the earlier QoL research. For example, for overall quality of life, there was a nearly 20% increase in the number of hearing aid users noting improvement.
A second research question dealt with the similarity between the ratings of the participant and their significant other, based on his or her observations of the participant; how they believed the participant should rate the item. These comparative findings are shown in Figure 2. Observe that, in general, the overall findings are very similar; the person’s correlation was .90 or greater (p<.001) for all items.
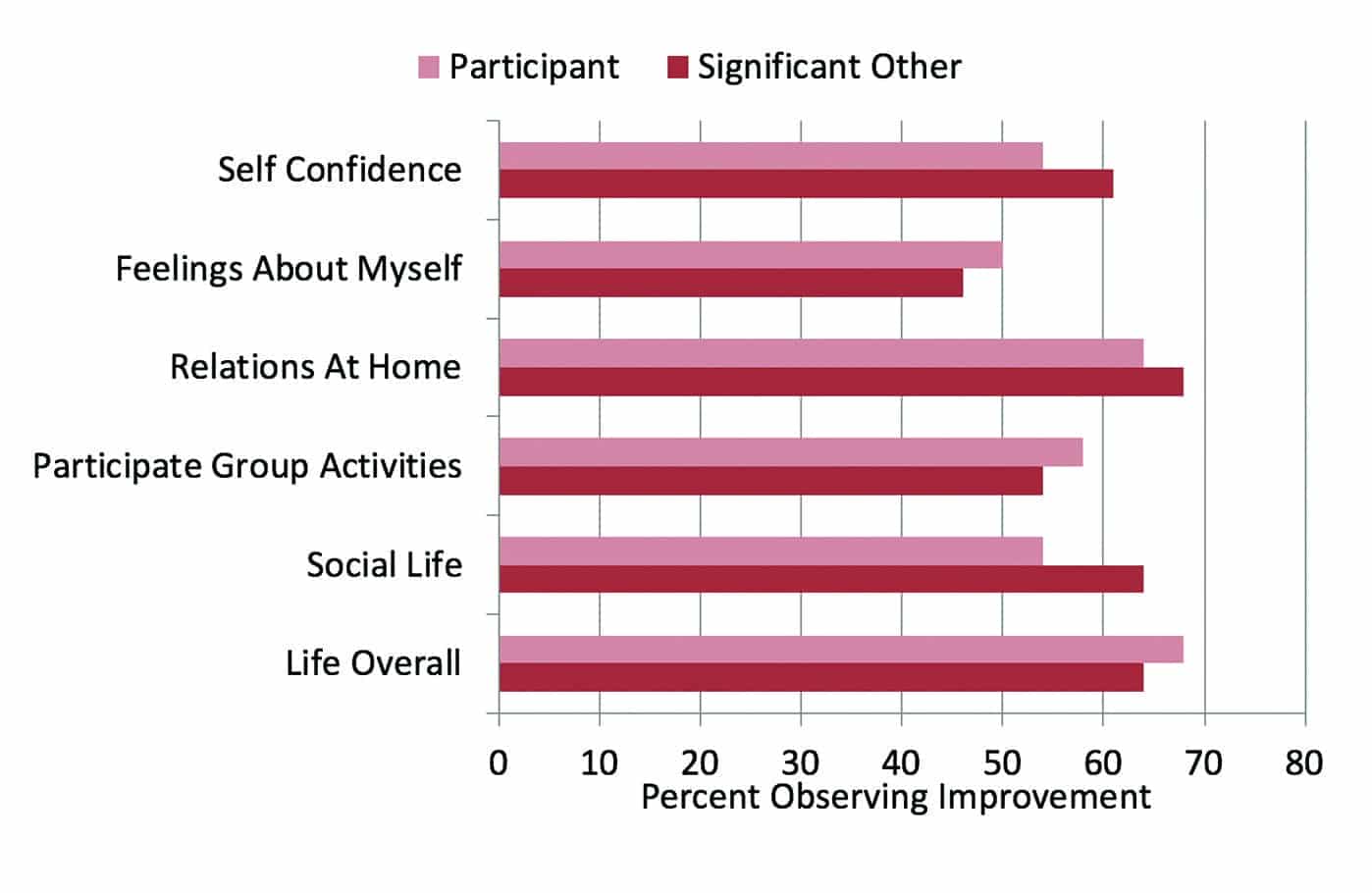
Figure 2. Shown are the percentage of participants who reported at least “Some Improvement” for the different quality-of-life items. Shown for comparison are the findings from the significant other of each participant, who answered the same survey questions as they believed the hearing aid user should answer.
The NCOA survey showed a trend for slightly higher ratings for the significant other than those of the hearing aid user, which we only observed for some dimensions. Perhaps this was because of the relatively short time our participants had used their hearing aids (6 weeks), and therefore, the significant other only had limited observations. The similarity in the ratings between the participants and their significant others, however, does suggest that we were not observing an experimental bias with our participants that may have caused them to elevate their ratings (eg, a Halo or Hawthorne effect).
We also were interested whether the participants’ ratings on the QoL questionnaire agreed with their COSI ratings. Recall that each participant had selected at least three situations where they believed they could participate more in conversations. The hearing aids used in the study had the new OVP algorithm, previously shown to encourage more communication.8 Shown in Figure 3 is a scatter plot of the COSI rating (y-axis; 1 to 5 scale) as a function of the individual participant’s rating for improvement for overall quality of life (x-axis; also a 1 to 5 scale). The COSI rating shown is the average of the top two situations nominated by the participant. The size of the circle represents the number of participants for that data-point combination.

Figure 3. Shown is the relationship between each individual’s average COSI score (y-axis: 1 to 5 rating) compared to their quality-of-life improvement rating (x-axis: 1 to 5 scale). The size of the circle represents the number of participants for that data-point combination.
As apparent in Figure 3, there was a strong association between the COSI rating and the participants’ view regarding their overall improvement in quality of life since using the hearing aids; Pearson’s correlation between the two measures was 0.72 (p<.01). One can also see that all 10 the participants who had a QoL rating of #4 or #5, also had an average #4 or better rating for their COSI items. There was only one individual who had a relatively high COSI rating (#4 or better) who did not report an improvement in overall quality of life. Conversely, of the 6 participants who had an average COSI rating of #2 (“Same”), 5 of these also had a QoL improvement rating of #2 (“Same”).
Discussion
In general, the findings of this research reveal that the Signia Nx hearing aids equipped with OVP improve quality-of-life issues for the majority of new hearing aid users. This finding was supported by the ratings of the significant others. For most of the areas studied, the findings from this research show a significantly greater percent of improvement than what was reported by the large NCOA study. The EuroTrak 2015 (ET 2015)5 and MarkeTrak 9 (MT9)6 worldwide studies also examined some of the non-auditory benefits of amplification. One of the findings from their work was that a significant percent of hearing aid users stated that hearing aids improved their relationships at home; 44% in the US, and an average of 51% for five European countries. Our data (see Figure 1) revealed that 64% of the new hearing aids users reported improvement of relations at home—20% higher than the reported US average.
We also need to point out that the participants in this study had only been fitted with hearing aids for 6 weeks. It’s reasonable to believe that quality of life improvement would continue to increase as the duration of hearing aid use was extended and the hearing aid users had more life experiences using amplification.
Recall that the participants in this study were a sub-sample of a larger research project regarding the use of Signia’s new OVP.8 As part of that study, individuals selected key communication situations where they would like to be more active in the conversation. The notion was that if a person’s voice sounded “natural” with new amplification, they would be more likely to talk. This proved to be true. The results revealed increased participation for 75 of the 96 communication settings nominated (78%), with 28 (88%) of the 32 participants reporting increased communication in at least one of the three situations that they selected.8What we have learned from the data in our current analysis is that there is a significant association between communicating more and improvement in various areas related to quality of life (see Figure 3).
Conclusion
Our findings reveal that modern hearing aid technology improves the patients’ quality of life to a greater extent than shown in previous studies. While it is not possible to determine the degree of the direct relationship, it appears that OVP leads to talking more in important communication situations, and in turn, this helps lead to the improvement. The large improvement noted for “group activities,” known to be noisy, certainly could be the result of recent advances in noise reduction and bilateral beam forming. All clearly showing that hearing aids do more than just improve hearing, and indeed, “Better Hearing is Better Living.”

About the Authors: Thomas A. Powers, PhD, is the Managing Member of Powers Consulting and Chief Audiology Consultant for Sivantos Inc; D. Bradley Davis, AuD, is an educator and clinical audiologist at the University of Arkansas at Little Rock/University of Arkansas for Medical Sciences specializing in hearing instrument fitting and aural rehabilitation; Matthias Froehlich, PhD, is head of Audiology Marketing at Sivantos GmbH in Erlangen, Germany; and Amyn Amlani, PhD, is the Professor and Chair of the Department of Audiology and Speech Pathology in the consortium program between the University of Arkansas Medical Sciences and the University of Arkansas at Little Rock.
CORRESPONDENCE can be addressed to Dr Powers at: [email protected]
Citation for this article: Powers TA, Davis B, Froehlich M, Amlani AM. Better hearing is better living. Hearing Review. 2019;26(1)[Jan]:18-20.
References
-
Chisolm TH, Johnson CE, Danhauer JL, et al. A systematic review of health-related quality of life hearing aids: Final report of the American Academy of Audiology Task Force on the Health-Related Quality of Life Benefits of Amplification in Adults. J Am Acad Audiol. 2007;18(2):151-183.
-
Ferguson MA, Kitterick PT, Chong LY, Edmondson-Jones M, Barker F, Hoare DJ. Hearing aids for mild to moderate hearing loss in adults. Cochrane Database of Systematic Reviews. 2017;9(CD012023):1-48.
-
Kochkin S, Rogin CM. Quantifying the obvious: The impact of hearing instruments on quality of life. Hearing Review. 2000;7(1):6-34.
-
Untreated hearing loss linked to depression, social isolation in seniors. Audiology Today. 1999;11:(4).
-
Hougaard S, Ruf S, Egger C, Abrams H. Hearing aids improve hearing–and A LOT more. Hearing Review. 2016;23(6):14.
-
Abrams HB, Kihm J. An introduction to MarkeTrak IX: A new baseline for the hearing aid market. Hearing Review. 2015;22(6):16-22.
-
Lentz WE. Speech discrimination in the presence of background noise using a hearing aid with a directionally sensitive microphone. Maico Audiologic Library Series. 1972;10(9).
-
Powers TA, Davis B, Apel D, Amlani AM. Own voice processing has people talking more. Hearing Review.2018;25(7):42-45.
-
Høydal EH. A new own voice processing system for optimizing communication. Hearing Review. 2017;24(11):20-22.
-
Powers T, Froehlich M, Branda E, Weber J. Clinical study shows significant benefit of own voice processing. Hearing Review. 2018;25(2):30-34.
-
Froehlich M, Powers TA, Branda E, Weber J. Perception of own voice wearing hearing aids: Why “natural” is the new normal. Audiology Online. April 30, 2018.
-
Dillon H, James A, Ginis J. Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J Am Acad Audiol. 1997;8:27-43.