

Cochlear implantation in children has typically been performed on those who derive minimal or no benefit from conventional amplification. Once implanted, in most cases these children are advised to discontinue use of their hearing instrument worn in the opposite ear, since speech perception skills in implanted children have been shown to be significantly better than those using hearing instruments with comparable hearing losses.1-3 The assumption made in the past was that use of a cochlear implant in one ear and a hearing instrument in the other ear was not indicated because performance measures showed the cochlear implant outperforms the hearing instrument in most cases, and thus would present asymmetrical inputs to the auditory system.
There is some research basis for this assumption, at least for binaural hearing instrument use. In a study by Hood & Prasher4, it was reported that patients with bilateral sensorineural hearing loss who have dissimilar cochlear distortion in both ears, may have poorer word recognition scores with a binaural fit than their best monaural word recognition scores. Their assumption was that the cortex may be unable to contend with the incongruent signals coming from the two ears with dissimilar auditory function. This study, however, utilized normal subjects who were used to receiving similar binaural signals, and potential learning effects over time were not explored. As Gatehouse & Killion5 pointed out, “…there is a fundamental perceptual process whereby a hearing impaired listener, when presented with a range of speech information which had been previously unavailable, can take considerable time to learn to make optimum use of the new set of speech cues and thereby derive optimal benefit from the amplification.”
The advantages of binaural amplification and binaural hearing have been well documented using both subjective and objective measures. Some of the reported benefits include:
- Enhanced localization ability;
- Improved overall speech clarity;
- Better speech discrimination in noise and quiet;
- Lower gain requirements for each hearing instrument resulting from binaural supra-threshold loudness summation;
- More relaxed listening ability.6-12
Despite these reported binaural advantages, there have been no definitively established criteria for appropriate binaural candidacy. This is a unique problem, especially where a hearing aid is to be used in one ear and a cochlear implant in the other.

Fig. 1. Audiogram for ES.

Fig. 2. Speech perception test results for ES.
Some researchers have attempted to establish candidacy guidelines for binaural hearing aid fittings. For example, Berger & Hagberg13 suggested that binaural fittings are indicated:
- If the dynamic range and the UCL of each ear are within 15 dB;
- If word recognition scores at the same sensation levels are not significantly different, and
- If pure tone thresholds differ by no more than 15 dB at any of the speech frequencies and are essentially equivalent.
They also recommend that some “reasonable degree of symmetry between two ears points to probable binaural success.” Davis & Haggard14 recommend binaural fittings be made when the average thresholds of both ears are within 12 dB of each other from 500-4000 Hz.
While most guidelines recommend binaural symmetry as a prerequisite to binaural hearing instrument fitting, Erdman & Sedge9 and Johnson15 did not find asymmetry necessarily to be a factor contraindicating binaural fitting. Mueller16 indicated that establishing some arbitrary numerical cut-off point for determining binaural candidacy may impede the professional’s task when determining the optimal hearing aid fitting arrangement. Byrne & Dermody17 reported that a good reason to fit asymmetrical losses binaurally is to achieve what they called a “crossover” effect. That is, when each ear has a different range of frequencies to which it responds better, a binaural fitting may result in a wider range of frequencies being presented to the auditory system than would be presented by either ear alone. Thus, a more effective fitting might result.
A compelling argument for consideration of binaural fitting can be found in a recent study by Gelfand & Silman.18 They suggest that monaural hearing instrument fitting may result in an auditory deprivation effect in the non-amplified ear. They investigated children with bilateral moderate sensorineural hearing losses after four years of hearing aid use, with one group amplified monaurally and one group amplified binaurally. Those children aided monaurally had significantly poorer word recognition scores for the unaided ear compared to their initial test performance. In contrast, the word recognition scores in the aided ear did not decrease from original performance for either the monaurally aided or the binaurally aided patients.
As Briskey19 suggested, the ability to achieve a balanced sensation should be the critical factor when fitting patients binaurally, and the potential advantages of binaural amplification should be pursued beyond some arbitrary binaural fitting criteria. Perhaps the question should not be whether binaural use of amplification is better than monaural, but whether binaural fusion can be achieved, especially when considering use of a cochlear implant in one ear and hearing aid in another, where different input signals are presented to both ears.
Since the majority of the research on binaural hearing has been done on patients using two comparable amplification systems (i.e., binaural hearing instruments), little is documented on the potential binaural benefits of combining a hearing instrument with a cochlear implant, especially in children. Waltzman et al20 reported on eight adult patients who were evaluated while using two hearing aids (no CIs), two cochlear implants and with both CIs and hearing aids together. They concluded that use of both devices together can provide improved speech perception ability for adults over monaural use of either alone. There is little published data regarding the use of cochlear implant and hearing instruments in children.

Fig. 3. Audiogram for JA.

Fig. 4. WIPI closed-set test for JA.
In the early days of cochlear implantation, it was not as critical to consider binaural fitting, since the patients were typically so profoundly deaf that, even when aided, they were barely able to detect presence of sound, let alone understand any speech. Now that medical centers are implanting patients who do achieve some pre-operative word recognition ability with their hearing aids21, it becomes necessary to assess whether they would derive additional benefit by continuing to use a hearing instrument in the opposite ear. This is even more important in pre-linguistically deafened children during their critical language-learning years. It is well known that children who have access to a greater number and variety of acoustic cues have an easier time developing appropriate listening skills and ultimately developing better speech production skills. If these disparate signals can be blended to achieve binaural fusion, it might allow them more access to this important auditory information.
This paper will present speech perception results on four patients who use a cochlear implant in one ear and a hearing instrument in the other. The case studies involve two patients who were pre-linguistically deafened and two who were post-linguistically deafened.
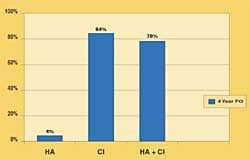
Fig. 5. PBK-50 words (open-set) for JA.
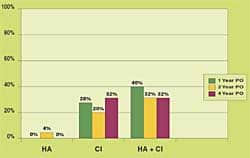
Fig. 6. CID sentences (open-set) for JA.
Case Studies
- Case 1: ES, 7-year-old male: ES was diagnosed with congenital genetic sensorineural hearing loss at 12 months of age. The loss was originally determined to be of moderate-severe degree and he was fit with binaural hearing aids. By age two, the loss had progressed to a profound degree bilaterally. His hearing aids no longer provided him with sufficient benefit for auditory/oral communication, so at two years of age he was implanted with a Nucleus 22 multi-channel cochlear implant in his poorer hearing (left) ear. He has been educated in an oral classroom and currently attends a regular education second-grade classroom.
- Fig. 1 shows his unaided audiogram and aided audiogram with the hearing aid and cochlear implant. While the aided thresholds with the cochlear implant and hearing aid at 250 and 500 Hz are essentially the same, his high frequency thresholds are measurably better.
- Speech perception testing, shown in Fig. 2 confirms the benefits of this enhanced access to high frequency spectral information via the cochlear implant. Open-set word recognition ability was evaluated using PBK-50 monosyllabic words and CID sentences. He was tested in the sound field in three conditions: hearing aid alone, cochlear implant alone and both devices together at his three and four year post-operative intervals. Results for PBK-50 words revealed that, with the hearing aid alone, he had only an 8% word recognition ability at three years and 4% at four years post-operation. In contrast, with the cochlear implant alone, he was able to correctly repeat 80% of words at three years post-op and 86% at four years. In the binaural condition, his word recognition score at three years was 88% and 94% at four years. The same pattern was seen using CID sentence materials. He correctly repeated 25% of the words with his hearing instrument alone at three years and 4% at four years post-op. With his cochlear implant alone, he achieved a score of 95% at three years and 98% at four years, and with both together, his score was 100% at both post-operative intervals.
- Subjectively, he indicated a preference for wearing both the cochlear implant and hearing aid together for several reasons. First, he reported that speech appears to be heard in the middle of his head rather than in either ear. He also reported that wearing both devices provided added security if either were to stop working during the school day. Clearly his cochlear implant outperformed his hearing aid, even after four years of continual use with both devices. With both the cochlear implant and hearing instrument worn together, there was a sight improvement in speech perception ability over the monaural use of the cochlear implant, and significant improvement over hearing instrument use alone.
- Case 2: JA, a 16-year-old male: JA was diagnosed with bilateral sensorineural hearing loss resulting from spinal meningitis at 10 months of age. He was fit with binaural hearing aids at 12 months of age and was enrolled in an auditory/oral educational program starting at age three. He currently attends regular high school with itinerant support services as necessary. At 11 years of age he received a Nucleus 22 cochlear implant in his poorer-hearing (left) ear, with the hope that he might have more access to sound to improve his speech perception and production abilities.
- Fig. 3 shows his unaided and aided audiograms for both the ear with the cochlear implant and the ear with the hearing aid. His aided results for the right ear and left ear are comparable for 250-1000 Hz. However, the high frequency thresholds with his cochlear implant are measurably better than those with his hearing instrument.
- Figs. 4-6 display his speech perception results in three conditions: hearing aid alone, cochlear implant alone and both worn together, at several post-operative test intervals. Fig. 4 shows the results for the closed-set WIPI test at 6 months, 1 year and 2 years post-op. With his hearing aid alone, he was able to correctly identify 36%, 32% and 44% respectively of the pictures over time. With his cochlear implant alone, he correctly identified 72%, 64% and 80%. With both the cochlear implant and hearing aid worn together, his scores were 84% at each test interval.
- A similar pattern of results emerged with the two open-set word recognition test measures (i.e., PBK-50 words [Fig. 5] and CID Sentences [Fig. 6]), evaluated at the 1-, 2- and 4-year post-operative intervals. With his hearing aid alone, he was unable to repeat any monosyllabic words at the 1- and 4- year intervals and 4% at the 2-year interval. With his cochlear implant alone, he achieved a score of 28%, 26%, and 32% respectively over time and with both devices together his scores were 40%, 32% and 32%. While his cochlear implant alone and cochlear implant and hearing aid word recognition scores for monosyllabic words revealed modest performance, they were both better than with the hearing aid alone, even after four years. He also was late in being implanted (i.e., age 11), which typically results in poorer open-set word recognition ability compared to those children implanted young.22,23
- Case 3: TH, a 7-year-old male: TH was identified as moderately hearing impaired at 17 months of age. The etiology was large vestibular aqueduct syndrome (LVAS). He was fit with binaural hearing instruments within three months of diagnosis and derived a significant amount of aided benefit. His hearing was stable until age five, when the progression began and by age six, the loss was severe to profound bilaterally. He was no longer able to function in a regular education class and was placed in a self-contained classroom for the hearing impaired. Prior to the progression, his speech was reported to be excellent and his language ability at grade level. Within six months of the progression, speech production and perception abilities were deteriorating and the decision was made to implant his poorer-hearing (right) ear with a Nucleus 24 cochlear implant.
- Fig. 7 shows his unaided and aided audiograms for both ears. Unaided thresholds are shown for both 1994 and 1997, which demonstrate the progression of the hearing loss. In his hearing aid ear, the aided threshold results reveal some low frequency benefit. However, with his cochlear implant ear, aided thresholds are better throughout the entire frequency range (250-6000 Hz). Fig. 8 shows his speech perception results both pre-operatively with his hearing aid and cochlear implant results at the four- and nine-month post-operative intervals. Three measures of open-set word recognition are reported (i.e., LNT words, PBK-50 words and BKB sentences). With his cochlear implant alone, there was a measurable improvement on all three tests by the four-month post-operative interval over the pre-operative hearing aid function.
- Testing with both devices together does not reveal any measurable improvement or decrement in word recognition ability over cochlear implant function alone. There is subjective preference for using both the hearing aid and cochlear implant worn together. Also to be noted is the rapid rate of improvement in speech perception skills, probably due to previous linguistic competence prior to the progression of the hearing loss.
- Case 4: ES, an 8-year-old female: ES was identified as having moderately severe hearing impairment at 15 months of age. She was aided bilaterally and performed well in regular education with minimal itinerant support services. However, at 7-years-old, she began experiencing episodes of vertigo, nausea and progressive hearing loss, which was worse in the left ear.
- The diagnosis was a presumed auto-immune disorder of the inner ear. After medical treatment, the vertigo subsided; however, the increased hearing loss persisted, and hearing levels progressed into the severe-to-profound range bilaterally. She was having extreme difficulty both educationally and socially and, at 7-years-old, was implanted with a Nucleus 24 cochlear implant in her poorer-hearing (left) ear.
- Fig. 9 shows her aided and unaided thresholds for both ears, and also reveals the progression of the hearing loss bilaterally. In her hearing aid ear, her aided audiogram ranges from 40-60 dB from 250-6000 Hz. Her implant aided audiogram ranges from 25-40 dB at the same frequencies, thus giving her additional access to the entire speech spectrum, especially at soft conversational levels.
- Fig. 10 shows her speech perception results on three open-set word recognition tests (i.e., LNT words, PBK-50 words and BKB sentences at the three- and six-month post-operative intervals). By three months post-op, she had substantially improved in word recognition ability in the implanted ear over her best hearing aided performance. At the six month interval, results continued to improve: with both devices worn together, she achieved excellent results. She reported being able to successfully use the telephone again.
Fig. 6. CID sentences (open-set) for JA.
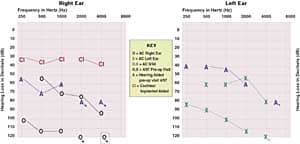
Fig. 7. Audiogram for TH.
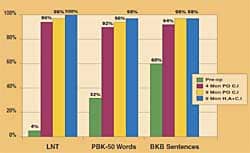
Fig. 8. Speech perception results for TH.
She notes that auditory information is best perceived with the cochlear implant, but she prefers the sound quality and localization ability afforded her with the use of both devices worn together.
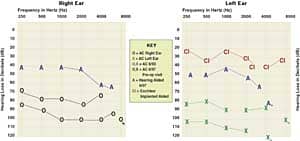
Fig. 9. Audiogram for ES.
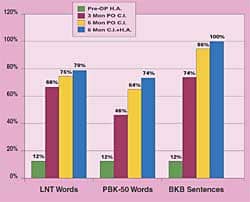
Fig. 10. Speech perception results for ES.
Discussion and Conclusions
In all four cases, implant aided function is measurably better than hearing aided function alone, especially in those patients who had some previous pre-operative open-set word recognition ability. The results with both devices worn together are similar to, or slightly better than, the cochlear implant worn alone. Formal testing has not demonstrated a clear functional superiority with the hearing aid and cochlear implant worn in combination. However many patients prefer this binaural condition, suggesting some subjective benefit is achieved that is not reflected by conventional test measures. The preference of some patients for binaural use of a hearing instrument in combination with a cochlear implant is not unlike some of the reported benefits that binaural hearing instrument users report, where a clear functional superiority cannot be demonstrated yet patient preference favors binaural device use.
There are clear perceptual differences reported by patients between the quality of sound heard through a hearing instrument versus a cochlear implant. Cochlear implants, by design, are intended to restore audibility of mid and high frequency sounds, essential for speech recognition. The hearing instrument may provide primarily low frequency cues at or near the fundamental frequency of speech, which may add more natural and improved sound quality. The combination of these acoustic features from both devices may be the contributing factor for patient preference and reported improvement in sound quality with the binaural use of the hearing aid and cochlear implant.
There may be some physiological basis for these quality differences as well. Recent x-ray studies have shown that typically the implanted electrode array is inserted in the 1 1/2-turns of the cochlea, thereby potentially minimizing some low-frequency apical cues. Whatever the differences, clearly a cochlear implant and hearing instrument can be combined to achieve increased patient benefit.
Another interesting finding can be seen when reviewing the speech perception data over time for Patients 1 and 2. Despite growth in language ability with age, their word recognition scores in the hearing aid ear did not improve while their scores in the cochlear implant ear continued to improve. In these two cases, the subjects effectively acted as their own controls (i.e., the same child in the same educational and social setting achieving different results in word recognition ability in each ear). This can only be explained by differences in device characteristics: the cochlear implant obviously giving the children greater access to sound, resulting in improved word recognition ability in that ear.
Results for Patients 3 and 4 (the post-linguistically deafened children) show a similar pattern to each other. Both had significant pre-operative benefit from hearing aids prior to the progression of their hearing losses and had “bonded” to their hearing aids. They each had initial adjustment problems to the new sound from the implant and relied heavily on their hearing aids for the first month after surgery. Within three months of bilateral device use, both patients demonstrated substantial improvement in speech perception skills in the implanted ear over their pre-operative function with their hearing aid, and both preferred to use the hearing aid and cochlear implant together for reportedly better sound quality.
Discussions with audiologists at other centers revealed that many recommend that their patients discontinue hearing aid use, at least for the first month, and learn to rely on the implant alone. Our post-linguistically deafened pediatric patients do not want to stop using their hearing aids. Even though the benefit with their hearing aid alone is minimal, they are accustomed to listening with that device, and rely on whatever cues are provided by their hearing aids. Our center recommends that the patients wear both devices together, but should spend some time with the cochlear implant alone each day, both during structured speech therapy and at home in their family environment. In our experience, the patients adjust to the new sound from the implant within one to three months and find that use of both devices together can result in a comfortably blended input signal.
As one teenage patient remarked after a few months of binaural device use, “my hearing aid is my friend; my cochlear implant is my friend; and now they are friends with each other.” w
References
1. Miyamoto RT Osberger MJ Robbins AM Myers WA, Kessler K & Pope ML: Comparison of speech perception abilities in deaf children with hearing aids or cochlear implants. Otolaryng Head and Neck Surgery 1991; 104 (1): 42-46.
2. Osberger MJ, Miyamoto RT, Robbins AM, Renshaw JS, Berry SW, Myers WA, Kessler K & Pope ML: Performance of deaf children with cochlear implants and vibrotactile aids. J Amer Acad Audiol 1990; 1 (1): 7-10.
3. Moog JS & Geers AE: Effectiveness of cochlear implants and tactile aids for deaf children: The sensory aids study at Central Institute for the Deaf. Volta 1994; 96 (5): 97-202.
4. Hood JD & Prasher DK: The effect of simulated bilateral cochlear distortion on speech discrimination in normal subjects. Scand Audiol 1990; 19 (1): 37-41.
5. Gatehouse S. & Killion M: HABRAT: Hearing aid brain rewiring accommodation time. Hear Instrum 1993; 44 (10): 29-31.
6. Carhart R: Monaural and binaural discrimination with competing sentences. Intl Audiol 1965; (4): 5-10.
7. Olsen W. & Carhart R: Development of test procedures for evaluation of binaural hearing aides. Bulletin Publish Research; Spring, 1967.
8. Erdman SA & Sedge RK: Subjective comparisons of binaural versus monaural amplification. Ear Hear 1981; 2 (5): 225-229.
9. Erdman SA & Sedge RK: Preferences for binaural amplification. Hear Jour 1986; 39 (11): 33-36.
10. Hirsch IJ: Binaural hearing aids. A review of some experiments. JSHD 1950; (15): 114-123.
11. Carhart R: The usefulness of the binaural hearing aid. JSHD 1958; (23): 41-55.
12. Hawkins DB: Hearing Aid Assessment and Use in Audiologic Habilitation, Third Edition. Ed. By William Hodgson. Baltimore: Williams and Wilkins, 1986: 142-143.
13. Berger KW & Hagberg EN: An examination of binaural selection criteria. Hear Instrum 1989; 40 (9): 44-46.
14. Davis A & Haggard MP: Some implications of audiologic measures in the population for binaural aiding strategies. Scand Audiol 1982; (Suppl) 15: 167-179.
15. Johnson EW: Binaural amplification-naturally. Hear Instrum 1987; 38 (12): 19-22.
16. Mueller HG. Binaural amplification: attitudinal factors. Hear Jour 1986; 39 (11): 7-10.
17. Byrne D & Dermody: Handbook of Clinical Audiology, Third edition. ed. Katz, 729.
18. Gelfand SA & Silman S. Apparent auditory deprivation in children: Implications of monaural versus binaural amplification. JAAA 1993; 4 (4): 313-318.
19. Briskey RF & Sandlin RE: Instrument Fitting Techniques. Hearing Instrument Science and Fitting Practices. Livonia, MI: National Institute for Hearing Instrument Studies. 1985: 471-475.
20. Waltzman S, Cohen N & Shapiro W: Sensory aids in conjunction with cochlear implants. Amer Jour Otol 1992; 13 (4): 308-312.
21. Larky J: Who is a cochlear implant candidate? Criteria for referring patients. Hear Jour 2000; 53 (6) 38-42.
22. Waltzman SB, Cohen NL, Gamolin RH et al: Long-term results of early cochlear implantation in congenitally and prelingually deafened children. Amer Jour Otol 1994; 1-4 (Suppl. 2): 9-13.
Marsha Simons-McCandless, MA, is director of the Univ. of Utah Cochlear Implant Program, and Clough Shelton, MD, is a physician at the Univ. of Utah Medical Center, Salt Lake City, UT.
Correspondence can be addressed to HR or Marsha Simons-McCandless, MA, Univ. of Utah Medical Center, 50 N. Medical Center Dr., Salt Lake City, UT 84132; email: [email protected].



